Polio at the Verge of Ending: A Big achievement
Dr. Shuvomoy Banerjee, PhD; from Neucrad Health desk, Sept. 1, 2020
The fight against polio began in 1950, when the first inactivated polio vaccine (IPV), developed by Dr. Jonas Sack (a leading scientist at the University of Pittsburgh, USA) got approved. 36 long years have passed since then and Polio vaccine research has led to a rapid decline in the total number of polio patients worldwide. Polio vaccine was especially needed to save the lives of millions of children. The Global Polio Eradication Initiative (GPEI) created in 1986 by the World Health Organization (WHO), the Gates Foundation, UNICEF, and other countries aimed to eradicate polio from the face of the earth. Their latest strategy i.e. “The Endgame” strategy is gradually phasing out the polio vaccine use program in the polio-free regions. Before going into the details, let’s take a closer look at the polio epidemic and the struggle of human-race against it.
Polio virus infection:
Polio is caused by polio-virus which is a RNA virus of the Picornaviridae family. One of the characteristics of this family of viruses is that they mainly infect vertebrates. The RNA genome of polio-virus consists of 7500 base pairs in total and there is no envelope around the protein capsid of the virus. The geometric structure of the capsid is icosahedral in nature and is composed of four types of proteins (VP-1, 2, 3, 4). A total of 3 serotypes of the polio-virus are found. Importantly, antibodies made against one specific serotype do not have the ability to develop resistance against another serotype.
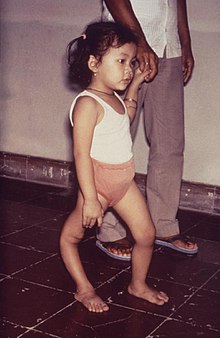
Polio-virus was first described in medical history around 1500 BC. One of the legs of a priest’s body in an ancient inscription of Rome was depicted unusually narrow and curved. Historical researchers believe that this feature of the body is definitely a symptom of polio. Subsequently, in 1909, two scientists, Landsteiner and Popper, first observed the transmission of the polio-virus. Their research demonstrated that the polio virus has the ability to permanently cripple vertebrates.
Interestingly, the polio-virus infects the human spinal cord and brainstem. The anterior horn of the spinal cord is severely damaged by this virus. The motor nerves in this region become useless and lose contact with the skeletal muscle. As a result, the muscles remain undeveloped and in some cases the patient becomes paralyzed (paralytic poliomyelitis).
Surprisingly, polio is predominant in children. Scientists have found that a child is not likely to get polio until the age of 6 months because the antibodies from the mother’s milk prevent the baby from being infected with the polio-virus. This is called ‘passive immunity’ against polio. However, the effectiveness of this immunity ends soon after that and the presence of polio-virus can be found in the stool. The polio-virus can enter the human body mainly through contaminated water, where it nests on the body’s nutrition system. From there onward, the virus penetrates the mucosal barrier and enters the bloodstream, attacking the central nervous system.
Polio vaccine discovery and its types:
Neutralizing antibodies are made in the body against 2 types of polio-virus antigens (antigens C and D). Among them, C antigen is the nucleic acid-free protein capsid of the virus and D antigen is the infectious virus conica containing protein capsid and nucleic acid. Two main types of vaccines have been developed to prevent polio virus infection as follows:
- Inactivated Polio Vaccine (IPV)- In 1950, Dr. Jonas Edward Sack developed the inactivated polio vaccine by chemically neutralizing the polio virus. Although this vaccine did well in early-stages of polio eradication programs, in some cases it was not able to develop complete immunity against polio.
- Live attenuated polio vaccine (OPV)- In the early 60s, Polish-American scientist Dr. Albert B. Sebin discovered the live attenuated polio vaccine from Cincinnati’s Children’s Hospital Research Foundation. This vaccine uses the active but non-infectious polio-virus. Surprisingly, it has much better results than IPV. However, the disadvantage of this vaccine is that the live attenuated polio vaccines cannot be properly maintained and transported in countries with a ‘tropical climate’ due to high average temperatures throughout the year which is the problem for maintaining the ‘cold chain’.
Worldwide Polio Immunization Program:
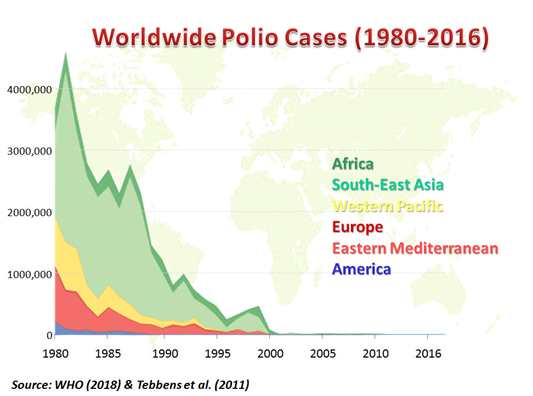
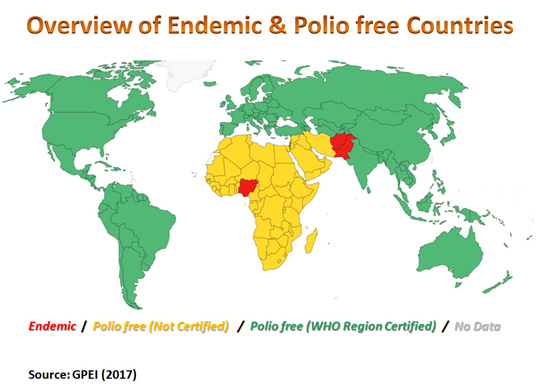
Since the discovery of IPV and OPV, there has been an active campaign to eradicate polio around the world. In the pre-polio vaccine era, the prevalence of polio was much higher in the regions adjacent to Africa, South Asia, Indian subcontinent than in western countries like Europe, America, Russia etc. Vaccine use has reduced polio infection rates by nearly a 1000 times, according to global studies! The program launched by the Global Polio Eradication Initiative in 1986 stated that the world will be polio-free by the year 2000. Since then, there has been an active drive to eradicate polio at various international levels, and in fact, by 2003 all countries of the world were declared polio-free except India, Nigeria, Afghanistan and Pakistan. In particular, the transmission of polio serotypes 2 and 3 is completely eradicated and only Serotype 1 is active. At present, very few polio infection data are remaining in the hands of researchers. Henceforth, “The Endgame Strategy” is adopted!

The Endgame Strategy:
In 2014, Southeast Asia (including India) was declared a “polio-free” region and in 2020 polio was eradicated from Nigeria. Currently, polio cases are being reported only from Pakistan and Afghanistan.
Of note, it was found that sometime the OPV gets released from the vaccinated child through faecal matters and can enter the body of healthy ones via faecal-oral route especially in unhealthy or contaminated environments, creating “circulating vaccine derived polio virus (cVDPV)” infection. This situation has been created in several developing countries of the world and appropriate measures have been taken to address it. As a result, collecting data for cVDPV infection became important along with polio serotype-1 infection data for the last stages of polio eradication.
Polio Endgame Strategy was launched whose main objective is to gradually phase out the administration and campaign of polio vaccination in polio-free areas based on collective data of cVDPV infection along with polio serotype-1 infection. The Polio Endgame Strategy requires regular monitoring, sample testing and survey. The current Polio Endgame Strategy of 2019-2023 initiative is a landmark step which mainly depends on 3 following goals:
- To arrange usage of controlled vaccines, regular surveys, data registration and data analysis through specific agencies in each country of the world.
- Delivering polio vaccine to every child globally in order to eradicate paralytic polio. Moreover, to make sure that there is no Wild-type Polio Virus (WPV) and Vaccine Derived Polio Virus (cVDPV) infection remaining anywhere.
- After critical review, declaring the polio-free country as “Certified Polio Free Country”.
The World Health Organization and the Global Polio Eradication Initiative have recently announced that “The achievement of polio eradication will be a milestone for global health“. Their statement has brought hopes as human-race is looking forward to a polio-free world soon.

References:
- https://www.who.int/health-topics/poliomyelitis#tab=tab_1
- http://polioeradication.org/
- Khan F, Datta SD, Quddus A, et al. Progress Toward Polio Eradication – Worldwide, January 2016-March 2018. MMWR Morb Mortal Wkly Rep. 2018;67(18):524-528. Published 2018 May 11. doi:10.15585/mmwr.mm6718a4
- Kalkowska DA, Duintjer Tebbens RJ, Thompson KM. Another look at silent circulation of poliovirus in small populations. Infect Dis Model. 2018;3:107-117. Published 2018 Jun 9. doi:10.1016/j.idm.2018.06.001
- Aylward B, Tangermann R. The global polio eradication initiative: lessons learned and prospects for success. Vaccine. 2011;29 Suppl 4:D80-D85. doi:10.1016/j.vaccine.2011.10.005
- Baicus A. History of polio vaccination. World J Virol. 2012;1(4):108-114. doi:10.5501/wjv.v1.i4.108
- Institute of Medicine (US) Vaccine Safety Forum; Howe CJ, Johnston RB, editors. Options for Poliomyelitis Vaccination in the United States: Workshop Summary. Washington (DC): National Academies Press (US); 1996. History and Current Status. Available from: https://www.ncbi.nlm.nih.gov/books/NBK231547/
- Bandyopadhyay AS, Garon J, Seib K, Orenstein WA. Polio vaccination: past, present and future. Future Microbiol. 2015;10(5):791-808. doi:10.2217/fmb.15.19
- Centers for Disease Control and Prevention (CDC). Progress toward interruption of wild poliovirus transmission–worldwide, January 2010-March 2011. MMWR Morb Mortal Wkly Rep. 2011;60(18):582-586.
- Chatterjee A, Vidyant S, Dhole TN. Polio eradication in India: progress, but environmental surveillance and vigilance still needed. Vaccine. 2013;31(9):1268-1275. doi:10.1016/j.vaccine.2012.12.060